


The sacrifices I make in the name of health prevention – plastering a photo of me in my pj’s ready for my sleep study on the internet!
It’s taken me over two years to write this blog on my own sleep apnoea diagnosis and subsequent treatment. I’ve been keen to do it but other blogs kept popping up and I just never got around to it. We know there is a strong link with nocturia and sleep apnoea, but at the gym today as I was watching the news, there was yet another headline about how sleep apnoea and dementia are linked and I was compelled to get off my butt and finally do it.
My story started when Bob (husband) decided to go to a sleep specialist a few months after we returned from our overseas trip in late in 2016. He had been struggling every night to stay awake much past 7pm and he felt like he had never got over his jet lag – and that was after 4 months. As I was sitting in with Bob at the respiratory physician’s appointment and she was asking him all the relevant questions, I had this overwhelming feeling that I should have been seeing her – not Bob!
Sleep apnoea, which means failure to breathe during sleep, can be obstructive or non-obstructive.
Non-obstructive or ‘central’ apnoea occurs when the brain fails to signal the breathing muscles that it’s time to get active.
In obstructive apnoea (also abbreviated to OSA standing for Obstructive Sleep Apnoea), breathing fails because of a relaxed airway that fails to open up despite the brain’s insistence. Eventually, sometimes after more than a minute without breathing, the brain sounds its alarms urgently enough to jolt the muscles of breathing back into action. Sometimes this wakes the sleeper, but more often the periods of apnoea and gasping serve only to rob sleep of its restful and restorative quality. A respiratory infection or excessive alcohol use can also interfere with breathing during sleep. Chronic and severe apnoea, however, is a prolonged, debilitating condition. (1)
After we sorted Bob (booked his sleep study) I chatted to the physician and she suggested that rather than coming to see her first, I just book straight in for a sleep study and after the study, come then to see her with the results. So Bob had his sleep study and got a clean bill of health and I went to Greenslopes Sleep Unit and they dressed me up (see photo at the top of the page) and I went back home to do my home sleep study. Like everyone, I naturally doubted I would sleep a wink trussed up as I was with the wiring and monitors, but it went swimmingly as I went to bed at 9.15pm and woke up at 6am having slept through the night without budging.
A week later I went to the doctor to read the results. It wasn’t pretty.
It had shown I had stopped breathing 27 times every hour; the longest pause in my breathing was 51 seconds and my oxygen saturation had dropped to 73% (it should be in the high 90’s). I was shocked to say the least. And so started the process of being assessed and fitted with a CPAP machine. CPAP stands for Continuous Positive Airways Pressure and is administered via a machine and a rather overwhelming mask and tubing – honestly my worst nightmare. More on that later. When working out mask types that are the most comfortable and give the best seal and pressures required to stop the sleep apnoeas, you have to go into hospital for the sleep study to trial their CPAP machine. I started with the nasal prong mask – and for me it was not good. It was quite uncomfortable. Then I moved onto the small half mask just over the nose, leaving the mouth free. My oxygen sats were much improved and the mask seal was good. The next step is to hire a CPAP machine for 4 weeks, returning weekly to assess the vital signs that these clever machines are able to report back to the team.
The first weeks were difficult because I suffer badly with claustrophobia. The first time I became aware of my ‘claustrophobia affliction’ was when I was about 19 and my mother paid for a single sleeper for my return train trip home from visiting my grandmother Dolly, who lived in Wollongong. The conductor diligently set up my bed at around 9 pm – but I lasted only half an hour before I called him again to return it to a seat. You see your face ends up about 6 inches away from the ceiling of the compartment and that freaked me out. This ‘claustrophobia affliction’ presented itself again on the first night we set up our campervan bed in Brighton on our first trip overseas together in 1984. Bob had taken quite a while to get it sorted (instructions were hard to come by) and again about 30 minutes after settling in, I literally jumped out of the bed and dived out of the van gasping for air. Again, my face 6 inches away from the roof was impossible for me to tolerate.
So you can understand that placing that mask over my head every night was my worst nightmare. I almost had to be asleep before I could tolerate it on – which is quite hard to master. Get the mask on and not fall asleep before that happened. By the end of week 2, I declared I just couldn’t do it. I had decided I was going to soldier on slowly destroying my brain cells without a CPAP machine.
And literally just then, the ABC News came on. Carrie Fisher, who played Princess Leia in the Star Wars series, had sadly died on a plane trip of sleep apnoea! I was shocked. I had never ever heard of sleep apnoea as a cause of death out loud on TV before. And just when I was being a complete idiot and denying the seriousness of my predicament, there it was – headline news.
I pulled up my Big Girl Pants and said get over your ‘Claustrophobia Affliction’ and make the bloody thing work – and I did and now my most favourite sleep companion (next to Bob) is my CPAP machine. From that moment it all went swimmingly. I suddenly had no trouble coping with it and my pressures, sats and mask fit were all stable and I proudly went back for my final visit to the team at CPAP Select at Greenslopes to buy my own machine. Luckily for me they had just had a brand new release of a Resmed Travel CPAP machine.

Resmed Travel Machine compared to the usual one
This machine is tiny compared to the one I thought I would have to buy and being much more portable than the big one I had been trialing would be great for our travels. It was a bit dearer at that time but I do believe they have come down in price these days. I am literally addicted to my machine now. I love it. I sleep completely through the night, never getting up anymore through the night and wake up refreshed and with clarity of thought (not that I really realized this until I had been using it for a few weeks). One night about a year ago we had a blackout and I literally thought I can’t go to sleep tonight until that power comes back on. I was scared to sleep flat without it.
It is very simple to set up and below is a You Tube video showing you how to use it.
[youtube https://www.youtube.com/watch?v=YlU28SvL2qs&w=560&h=315]
So why as a Pelvic Health Physio do I think is it so important to get yourself checked?
- decreased bladder capacity,
- reduced glomerular filtration rate and nocturnal polyuria due to decreased arginine vasopressin,
- incipient diabetes,
- sleep-disordered breathing, such as, obstructive sleep apnoea (OSA),
- congestive heart failure and/or diuretics use,
- benign prostatic hypertrophy in men
- vaginal atrophy with consequent reduced sphincter control in women.
Nocturia has been reported to be more severe in patients with OSA, and it is a well-researched end-organ symptom of OSA. It is found to be frequently associated with nocturia: 81% (17/21) women with OSA versus 40% (4/10) control women without OSA. The mechanism responsible for a higher prevalence of nocturia in OSA patients could be due to a reduced ability to concentrate urine during night sleep.
OSA is a condition characterized by repetitive episodes of complete or partial upper airway obstruction, which causes negative intra-thoracic pressure and consequently increases venous return to the heart. As a result, the right atrium and ventricle are distended, which receives wrong signaling of fluid overload, and the consequent release of brain-type atrial natriuretic peptide (ANP) from cardiac atria and ventricles. The secretion of anti-diuretic hormone (ADH), which is increased at night to promote the absorption of sodium and water from collecting tubules, is subsequently inhibited and this eventually leads to decreased urine concentration and consequent polyuria during night sleep.
In a study, diluted night-time urine was noted in 80% (16/21) of OSA patients, whereas it was noted in only 30% (3/10) of the control group. Numerous studies have reported reduction in nocturia after continuous positive airway pressure (CPAP) treatment in OSA patients, which supports the idea that OSA itself induces nocturia. However, despite the well-known pathophysiologic link between nocturia and OSA described above, the importance of nocturia has not been emphasized sufficiently in the context of screening for OSA. (The section in italics is taken directly from this article) (1)
But a second important reason is that people with sleep apnoea have been shown not only to have impaired memory and executive function, but also biomarker changes that are associated with Alzheimer’s disease. The results of several studies suggest that OSA might be a reversible cause of cognitive impairment and dementia, and that treatment of OSA, particularly in the early stages of AD, when patients are still largely independent, may decelerate dementia progression. (2) This particular article collected all available published clinical data and analyzed them through a quantitative meta-analytical approach. A quantitative meta-analysis suggests that the aggregate odds ratio for OSA in AD vs. healthy control was 5.05 and homogeneous. This reflects that patients with AD have a five times higher chance of presenting with OSA than cognitively non-impaired individuals of similar age.
And this is why I personally feel getting a sleep study should be a routine consideration once women are post-menopausal, especially if they snore, if they suffer with nocturia and if they feel exhausted initially on waking. There is a validated questionnaire called TANGO which is an easy check list with questions to see which domains are affected.
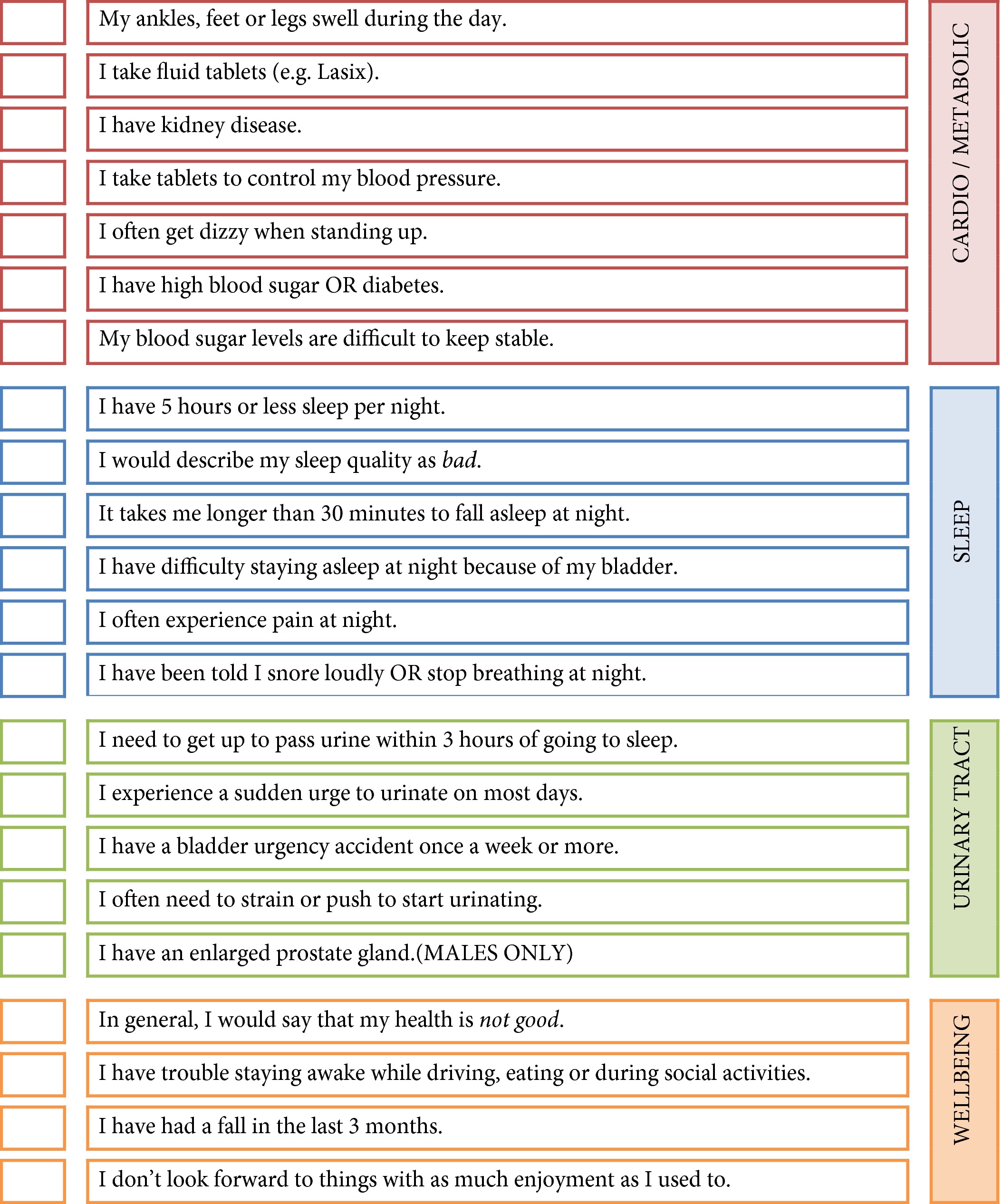{kind=link}
I hope through my own personal journey of sleep apnoea, I have de-mystified getting a CPAP machine and encouraged a few of you, if not quite a lot of people, to have their sleep study and when the results are not good, take the next step of trialing a CPAP machine.
It is definitely worth looking after your brain.
Now my next goal. Get to bed before midnight more often!
(1) Taken directly from: Park E et al (2015) Relationships between Nocturia, Obstructive Sleep Apnoea and Quality of Sleep, Sleep Medicine Research (SMR) 6(1): 28-34
(2)Emamian, F., Khazaie, H., Tahmasian, M., Leschziner, G. D., Morrell, M. J., Hsiung, G. Y., … Sepehry, A. A. (2016). The Association Between Obstructive Sleep Apnea and Alzheimer’s Disease: A Meta-Analysis Perspective. Frontiers in aging neuroscience, 8, 78. doi:10.3389/fnagi.2016.00078
Sue a very timely blog. Since I saw you last have been diagnosed with SIADH and have been wondering, well what caused this.
So will be looking at getting a Sleep Study done to see if any relationship is there.
Thanks for alerting us with these marvellous blogs.
.
Good idea Barb!